SUBMIT YOUR MANUSCRIPT
Affiliations
ABSTRACT
Cardiac metastasis from lung cancer as the first presentation is a relatively rare phenomenon and has a poor prognosis. Lung cancers can cause myocardial involvement through direct invasion, hematogeneous spread or lymphatic spread. Contrary to popular belief, cardiac metastases are not uncommon in oncology practice. Myocardial metastases are usually present in advanced stages of different cancer types and are only detected by imaging techniques. Cardiac magnetic resonance imaging (MRI) is the preferred imaging technique for the diagnosis and characterisation of cardiac masses. We report a case of lung cancer presenting with direct cardiac invasion evaluated with a transesophageal echocardiogram, computed tomography, and MRI. This report highlights cardiac metastasis as the rare initial presentation of lung cancer and the importance of detailed radiological evaluation in the differential diagnosis of cardiac masses.
Key Words: Cardiac magnetic resonance imaging, Cardiac metastasis, Lung cancer, Transesophageal echocardiogram.
INTRODUCTION
Despite advances in the diagnosis and treatment of lung cancer, it still ranks first in cancer-related deaths.1 At the time of presentation of lung cancer, common symptoms include cough, dyspnea, chest pain, fatigue, hemoptysis and weight loss.2 Tachycardia may not come to mind among the first causes suggestive of lung cancer. Herein, we report a case of squamous cell carcinoma of lung who was admitted to the emergency department with symptoms of fever, dyspnea, and tachycardia. On imaging findings, direct invasion of heart was confirmed.
CASE REPORT
A 45-year man, without relevant medical history, was admitted to the emergency department with a history of fever, dyspnea, and tachycardia. Arterial blood pH was 7.45 and pO2 was 50.1. He was an active smoker, with a 30-pack-year history of tobacco smoking. On chest X-ray, elevation of the left diaphragm was observed and a consolidated area was detected at the base of the left pleural hemithorax. A transesophageal echocardiogram (TEE) was performed with suspicion of thrombus or vegetation. TEE revealed a mass invading the left atrial posterior wall and causing thickening of the atrial wall.
At the same time, it was observed that the mass caused narrowing of the left upper pulmonary vein orifice. No vegetation and thrombus were detected (Figure 1). On the thoracic computed tomography (CT) and positron emission tomography (PET) scans, a left hilar mass invading the left pulmonary veins, left atrium, and atrial appendage was revealed. There was near total collapse with filling of the left hemithorax by pleural effusion (Figure 2). PET scan showed an increased metabolic activity in the mass whose borders could not be clearly distinguished, extending from the left hilar region to the left atrium.
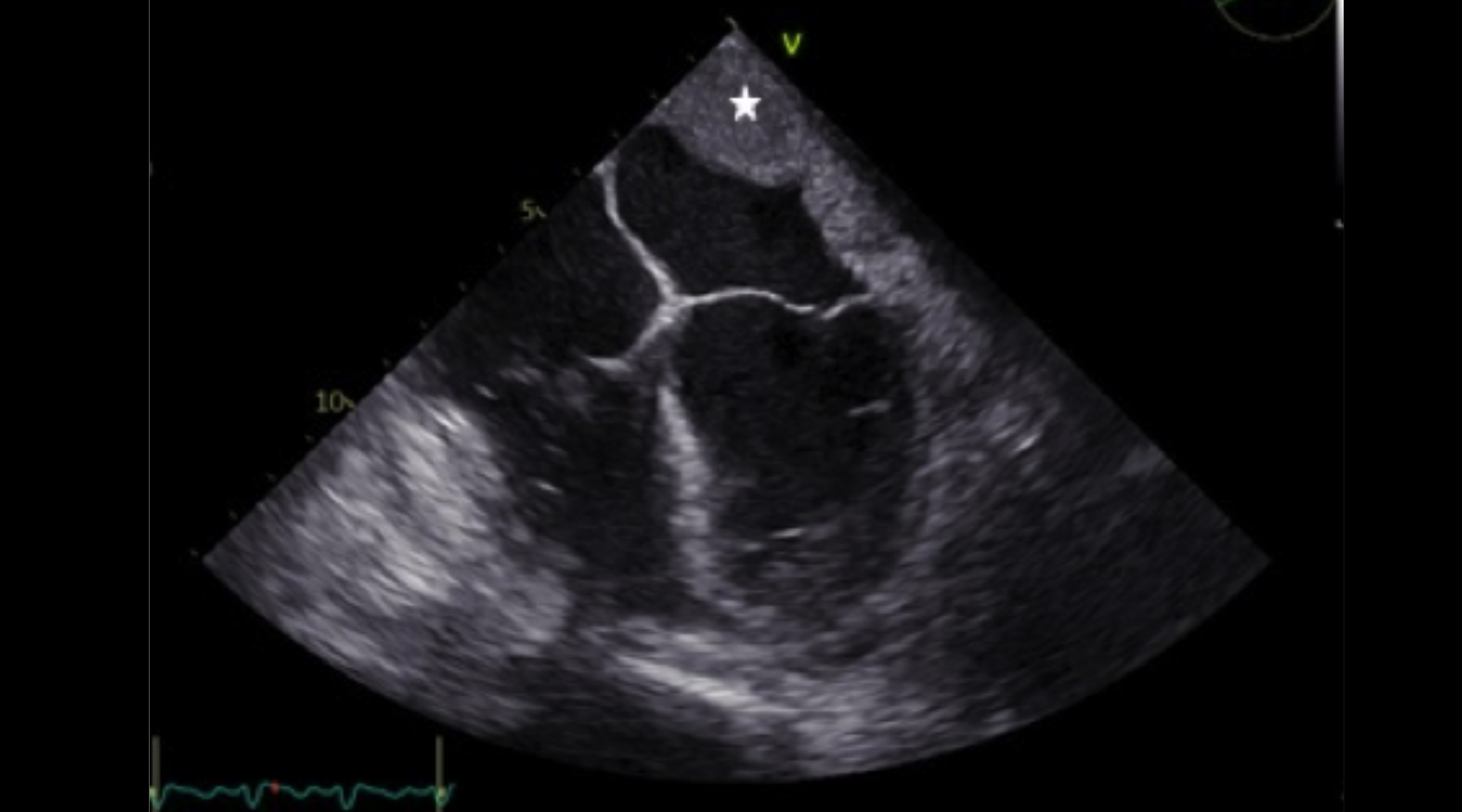 Figure 1: A transesophageal echocardiogram (TEE) image showing a mass (star) invading the posterior wall of the left atrium.
Figure 1: A transesophageal echocardiogram (TEE) image showing a mass (star) invading the posterior wall of the left atrium.
For further evaluation and differentiation of various aetiologies, cardiac magnetic resonance imaging (MRI) was recommended. On cardiac MRI, the left atrium from the posterolateral wall was invaded by the left hilar mass left pulmonary veins were also invaded and no flow signal was obtained (Figure 3). Findings on bronchoscopy and biopsy confirmed a diagnosis of squamous cell carcinoma, and the staging evaluation indicated stage IV disease. The patient received palliative chemotherapy to relieve his symptoms.
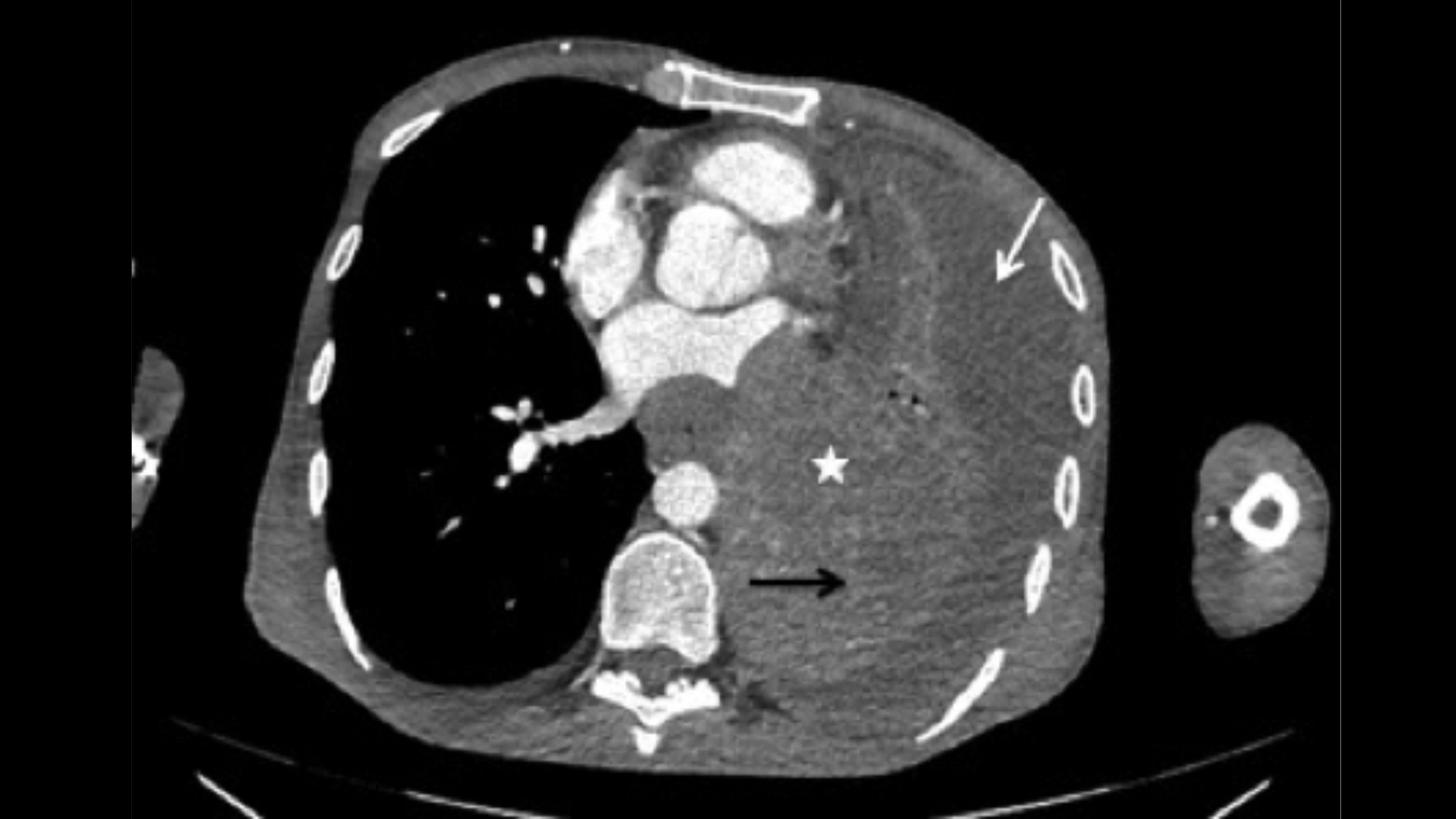 Figure 2: An axial CT image demonstrating a left hilar mass (star) invading the left pulmonary veins, left atrium and atrial appendage. Also, total collapse (black arrow) of the lung with filling of the left hemithorax by pleural effusion (white arrow) is seen.
Figure 2: An axial CT image demonstrating a left hilar mass (star) invading the left pulmonary veins, left atrium and atrial appendage. Also, total collapse (black arrow) of the lung with filling of the left hemithorax by pleural effusion (white arrow) is seen.
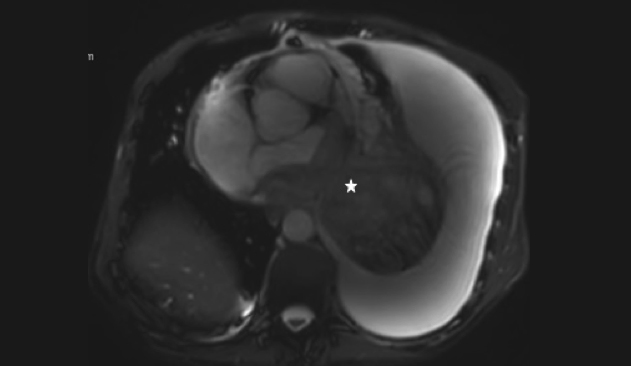 Figure 3: An axial cardiac MR image (SSFE) showing the heterogeneous mass (star) invading the left atrium and left pulmonary veins.
Figure 3: An axial cardiac MR image (SSFE) showing the heterogeneous mass (star) invading the left atrium and left pulmonary veins.
DISCUSSION
Cardiac tumours can arise directly from the heart. Sometimes, the heart may be involved by the spread of a nearby tumour, and at other times, by metastases from a distant tumour.3 While the metastases are by far the most common cardiac neoplasms, the primary cardiac tumours are very rare. The most common tumour type among primary cardiac tumours is myxoma. The other benign primary cardiac tumours are teratoma, rhabdomyoma, fibroma, papillary fibroelastoma, hemangioma, paraganglioma, and lipoma. Malignant primary cardiac tumours are rare and include angiosarcomas, pleomorphic sarcoma and leiomyosarcoma. Apart from the primary cardiac tumours, various malignant tumours can spread to the heart by metastasis. The leading causes of cardiac metastasis include pleural mesothelioma, melanoma, lung adenocarcinomas, squamous cell carcinoma of lung and breast carcinomas.4 In addition, it is possible for these tumours to show malignant character depending on their location and size. Therefore, effective use of imaging modalities in diffuse cardiac masses is important for accurate diagnosis and for tumour staging, prognosis, and appropriate treatment.5
Squamous cell carcinoma is a type of non-small cell lung cancer that most often occurs in the hilar region. Like other types of lung cancers, squamous cell carcinomas also present with typical symptoms. Some lung cancers may extend to the heart, which may be confused with atrial masses such as myxoma, vegetation, and thrombi. Whatever the cause, cardiac masses can lead to early death if undetected. Transthoracic echocardiography (TTE) is usually performed as the initial investigation in suspected cardiac mass. If the doubts about the nature of the detected mass are high and its invasion into the nearby tissue planes is suspected, TEE is applied. It can characterise the size, location and morphological features of the atrial mass.6 Recent studies have shown that cardiac MRI can also be used more widely for further evaluation.4,7
With the help of cardiac MRI, detailed analysis can be made about the volume of the heart, the force of contraction and its entire anatomy. Lack of ionising radiation, selection of multiplane images, tissue characterisation, perfusional status and myocardial movement assessment are other properties of cardiac MRI.8
In conclusion, lung cancers may occasionally present with direct cardiac invasion. Imaging techniques play important role in rapid and accurate characterisation of cardiac masses. This special case highlights the importance of cardiac MRI in diagnosing cardiac masses and detecting their aetiology. It also enables the determination of its relationship with both cardiac and extracardiac structures.
PATIENT’S CONSENT:
Written informed consent was obtained from the patient.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
ST: Conception and design of the work.
EKO: Editing and revising the manuscript critically.
SO: Acquisition and drafting of the work.
SDI: Performed the data analyses.
All authors approved the final version of the manuscript to be published.
REFERENCES